Why Motivation Won’t Fix Your POCUS Learning in 2026
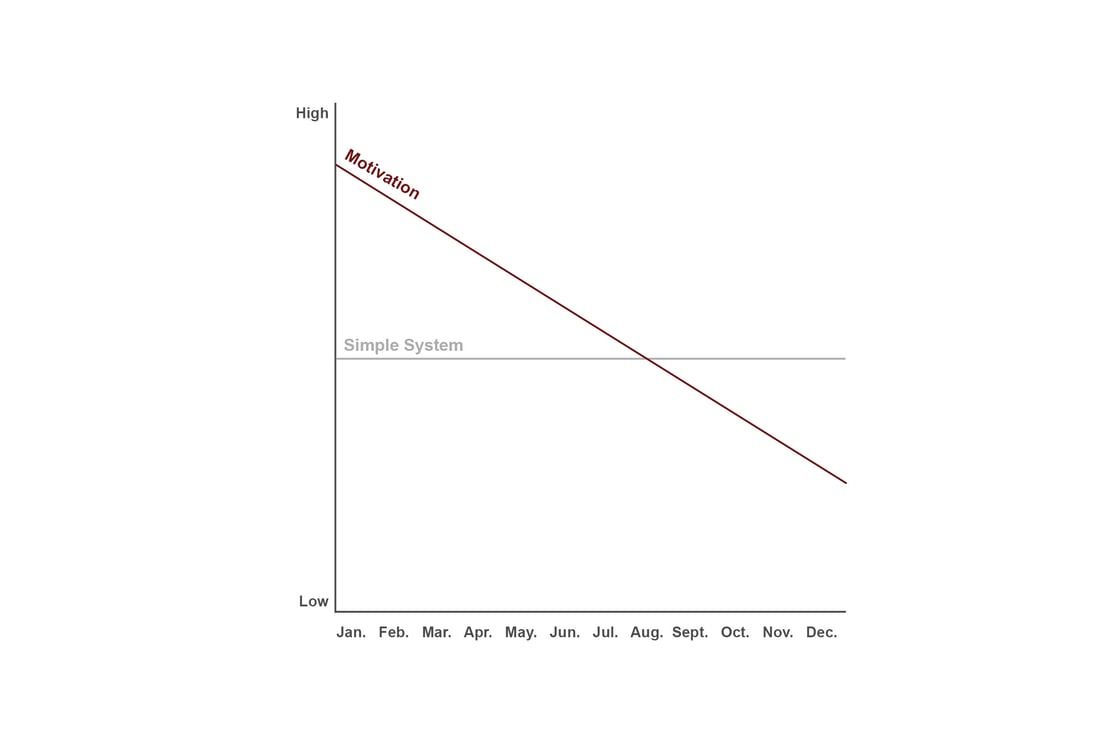
Motivation is a limited strategy for learning.
By now, we all know the uncomfortable truth about learning anything new.

And yet every January, we pretend this time motivation will carry us through. That wanting it badly enough will somehow override busy clinical days, cognitive load, and competing priorities.
Why This Keeps Happening (Even Though We Know Better)
If motivation were enough, most of us would be exceptionally fit, well-rested, and fluent in three languages by now.
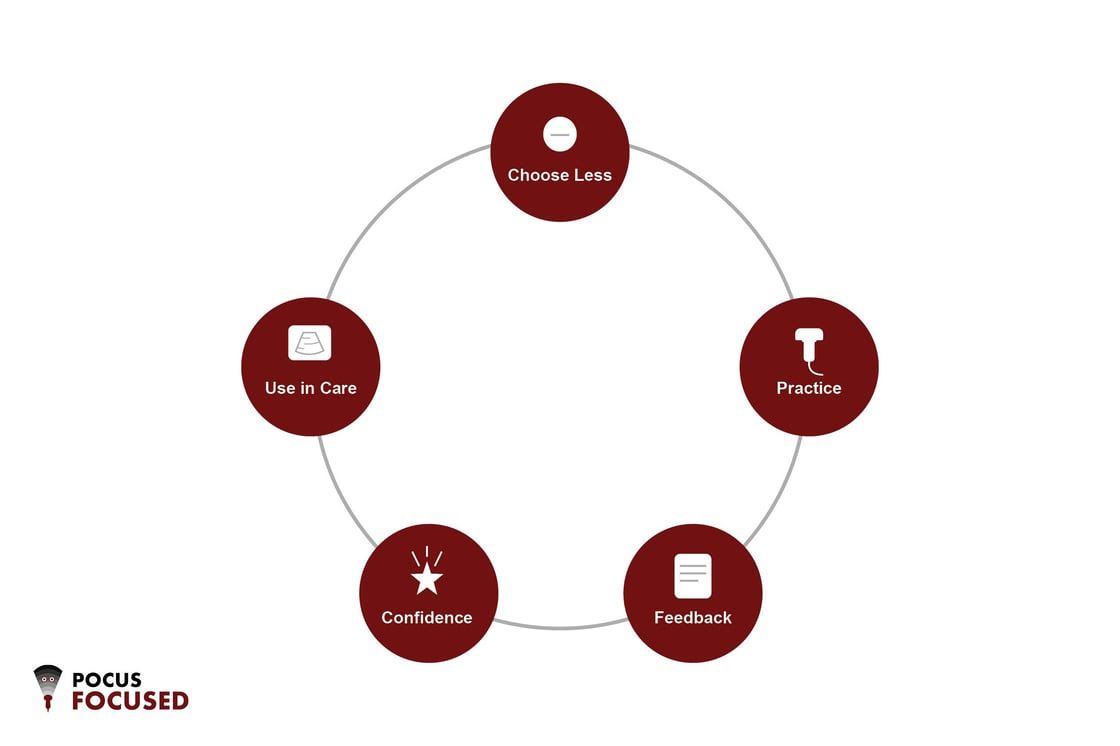
POCUS isn’t special in this regard. It obeys the same rules as every other durable clinical skill:
- small scope
- repeated exposure
- feedback
- clear signals of progress.
The problem isn’t that clinicians don’t know this.
The problem is that we keep designing learning plans as if we don’t.
The January Reset That Actually Works
Let’s do the counter-cultural ‘anti-January’ action instead.
The clinicians who truly integrate POCUS into practice aren’t just disciplined — they’re also more selective.
Putting This Into Action (Right Now)
Reading about better systems won’t change your POCUS practice. Designing one will.
One Focused 2026 POCUS Plan
Annual Objective: Develop reliable bedside ultrasound judgment for patients with undifferentiated dyspnea.
Quarterly Targets:
- Q1: Build a repeatable lung + focused cardiac scanning sequence; perform ≥25 scans
- Q2: Use POCUS findings to actively shape diagnostic reasoning and early management
- Q3: Refine efficiency and self-calibration; scan selectively and seek correlation
- Q4: Explain and teach dyspnea-focused POCUS decisions with confidence and restraint
One-Protocol Rule (this quarter):
Weekly 2-Minute Check-In:
Number of scans: ___
Protocol practiced: ___
- Confidence (0–10): ___
- Biggest friction point: ___
- One fix for next week: ___
Clinical Integration Target (by March):
Use dyspnea-focused POCUS during initial evaluation of patients admitted or evaluated for shortness of breath.
Your Turn
If this feels refreshingly manageable, that’s the point.
The One-Page 2026 POCUS Plan
Most POCUS learning plans fail because they ask clinicians to do too much, too soon.
This two-page worksheet is designed to help you choose one meaningful objective, define what progress actually looks like, and build a system you can sustain in real clinical life.
You’ll receive:
- A fillable one-page 2026 POCUS plan to clarify your annual objective and quarterly targets
- A companion worksheet of instructional prompts to help you choose deliberately and follow through
This isn’t a checklist or a curriculum.
It’s a simple framework for clinicians who want to stop dabbling and start using POCUS with confidence.
Talk soon,
Bob
Company
Learning
Connect
-
PO Box 23038Chagrin Falls, OH 44023
-
support@pocusfocused.com