Why POCUS belongs next to the stethoscope, not instead of it.
I've lost count of how many times someone has said to me, "POCUS is destroying the physical exam."
Sometimes it's joking, sometimes annoyed, and sometimes it's honest frustration with how the modern clinical encounter has drifted away from the bedside.
But I'll say this clearly: I disagree.
POCUS isn't the death of bedside skills. When used well, it brings clinicians back to the patient and sharpens the exam—not replaces it.
In my role as a clinical anatomy instructor working with first- and second-year medical students, I am adamant that your hands, eyes, and ears will always be your first diagnostic tools.
Ultrasound is powerful—but it comes after you've looked at the patient, talked to them, observed how they breathe, and touched the structures you're trying to understand. If you don't know the anatomy under your fingertips, the probe won't save you. It will just confuse you faster.
A Night in the ED
A middle-aged man arrived with shortness of breath, heart failure history, smoking history, recent long-haul flight. Could've been pneumonia, COPD, PE, acute decompensated HF, or just anxiety.
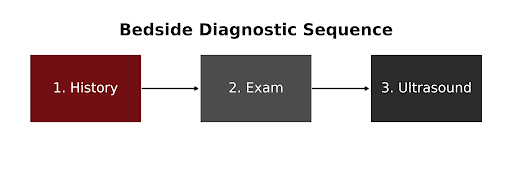
Instead of ordering everything at once, I started at the bedside:
Watched him breathe
Listened to his story without a keyboard between us
Checked neck veins, edema, lung and heart sounds
My working hypothesis: "This is heart failure until proven otherwise… but don't miss PE or pneumonia."
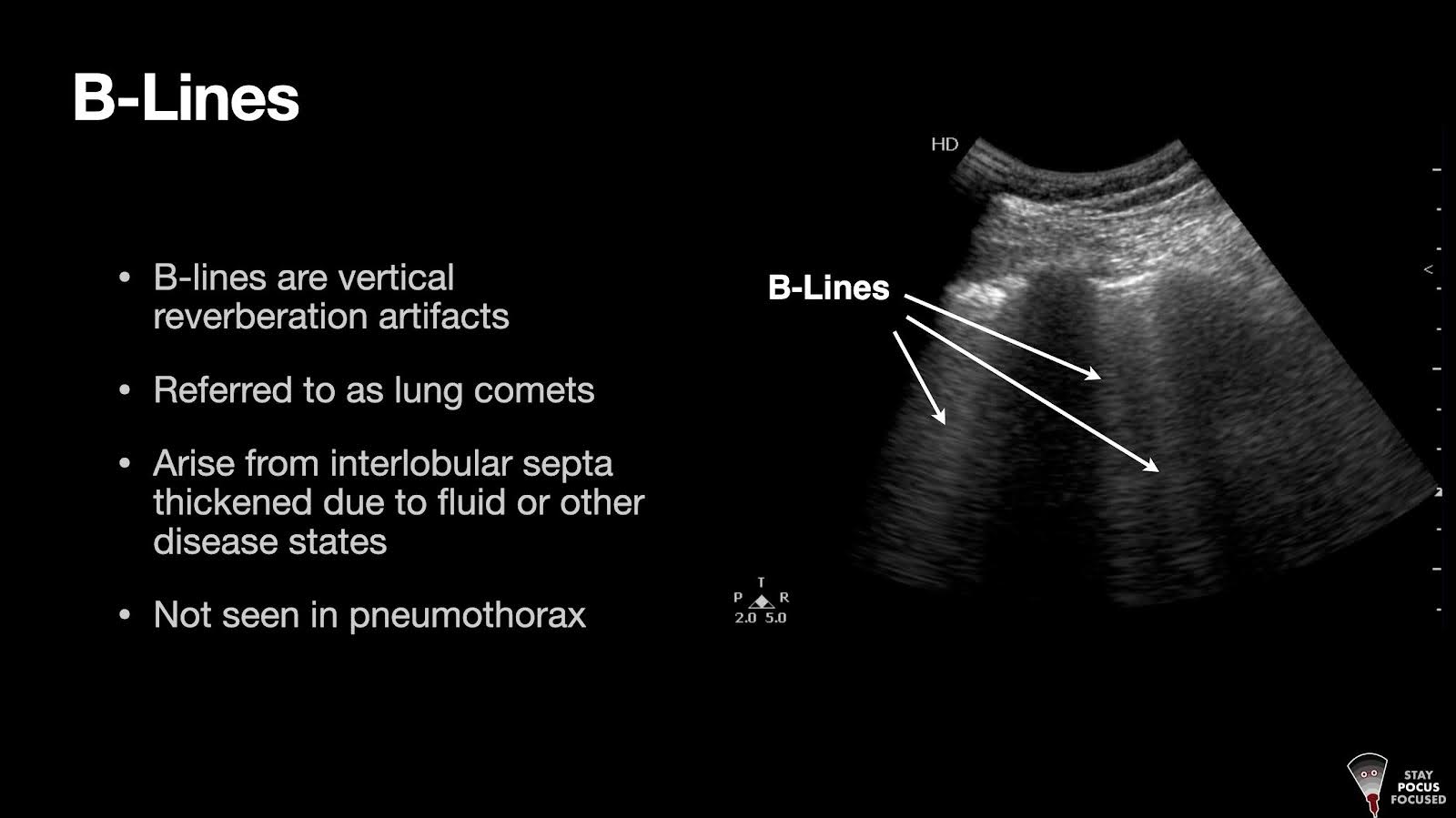
POCUS came last, to confirm and refine:
Write your awesome label here.
B-lines
Plethoric IVC
Reduced LV without RV strain
No unnecessary CT. Low diagnostic ambiguity. Fast, targeted therapy.
This is the pattern I've seen for decades: good clinicians use POCUS to close the loop on the bedside exam.
The National Conversation
Across medicine, there's renewed focus on the bedside encounter.
The Society of Bedside Medicine hosted its first annual conference earlier this month, dedicated to reinvigorating bedside skills, pairing traditional physical exam teaching with POCUS tracks.
A recent study in NEJM shows clinicians spend as little as 12% of their time in direct patient contact.
Two Myths We Need to Retire
Myth #1: Learners with POCUS will skip the physical exam.
Only if we teach them poorly.
The strongest medical schools teach in this exact order.
Myth #2: POCUS is just more tech pulling us away from patients.
The truth is that most tech that pulls us away is outside the room.
By contrast, POCUS keeps us present:
Hand on the patient
Eyes on the screen and the patient
Real-time dialogue about findings
Closing Reflection
I am not advocating abandonment of the stethoscope.
I am advocating for a return to the bedside—supported, not replaced, by ultrasound.
Consider these profound words by Dr Abraham Verghese, a national leader in the Bedside Medicine advocacy conversation. In his recent perspective, 'Culture Shock - Patient as Icon, Icon as Patient', which appeared in the NEJM, Verghese sums it up beautifully:
I feel fortunate to live in this age of incredible technology, with its remarkable new ways of seeing the body. I am excited about portable ultrasonography, for example, which allows us to instantly confirm findings at the bedside and discover the limits of our own skills. We need more of that kind of translational work — to develop the next generation of stethoscopes, ophthalmoscopes, and tendon hammers.
Surely, having physicians become more discerning, more comfortable, and eager to spend more time at the bedside is a good thing for patients. For the clinician, the bedside is hallowed ground, the place where fellow human beings allow us the privilege of looking at, touching, and listening to their bodies. Our skills and discernment must be worthy of such trust.
Call to Action
If this resonates with you, share this newsletter with 3 colleagues who care about bedside medicine.
PS: In the spirit of the season, we're opening a limited POCUS Focused Access Event this week — a short window with special first-month pricing and a set of new digital reference tools to support your bedside practice. Keep an eye on your inbox.
Heads Up: Part II Better at the Bedside coming next week
Learn how to build bedside mastery in 2025, with five habits you can start immediately.
Dr. Robert Jones, DO, FACEP— a nationally-recognized educator and front-line emergency physician — has dedicated his career to advancing POCUS from “novel tool” to standard practice. From launching ultrasound fellowships to authoring curricula and training thousands of clinicians worldwide, he blends over 30 years of high-volume trauma experience with proven teaching skill to shape the next generation of point-of-care innovators.
"Armed with the knowledge and techniques obtained from your school, I feel more equipped to navigate the challenging social aspects of the real world and become a professional in my field of choice."
Sue Porter
"I would definitely recommend your school to anyone hoping to pursue a career and be a professional. The support they provided to their students was simply outstanding and the genuine interest and care was obvious and incomparable."